

Resources
Radio personality Chilli Amar shares a personal journey of prevention, loss Read more about Chilli Amar's story.
Read more about Chilli Amar's story.New Survey Finds Women Know Little about GYN Treatments
Read more about the new survey and the importance of being your own advocate.New Survey Finds Women Know Little about GYN Treatments
Read more about the new survey and the importance of being your own advocate.Spotlight on Hysterectomies at WJLA’s Good Morning Washington with Dr. Paul MacKoul MD.
Watch Dr. Paul MacKoul MD on Good Morning Washington to learn about the basics of hysterectomies.National Cancer Survivors Day: Find a Support Group Early
There are many resources for women with gynecological cancers. Read more to find a support group near you.Minimally Invasive Surgery for Large Fibroids is Possible
Women with large fibroids, or an enlarged uterus are often told that they have no option other than undergoing a robotic or open procedures. Read more to learn about other procedures that are now available.Infographics
- Learn about DualPortGYN, a new minimally invasive gynecological surgery
- Learn about LAAM-BUAL, a new minimally invasive technique to remove large uterine fibroids, while leaving the uterus intact
- Wondering what the difference is between a gynecological generalist and specialist is?
- Get the facts on hysterectomies
- Get the facts on fibroids
{kind=link}
{kind=link}
{kind=link}
Third Party Websites


QUESTIONS TO ASK YOUR PHYSICIANS
How will the hysterectomy be performed and what is involved?
Sixty percent of all the hysterectomies performed in the U.S. are still open abdominal surgeries. This procedure can result in severe pain, higher complication rates, and a longer recovery period than new minimally invasive procedures. Other clinics use robotics, which require more incisions and more scarring. If your physician recommends these options, consider seeking a second opinion before agreeing to surgery.
How will my endometriosis be treated and what is involved?
First, if your physician recommends a hysterectomy, be sure to ask what other more conservative options are available to treat your symptoms if you would like to have children in the future. Depending on the severity of endometriosis, other surgical options exist such as endometriosis resection. If a hysterectomy is the right choice, you still have many options to consider. Sixty percent of hysterectomies in America are still open abdominal surgeries. This procedure can result in severe pain, higher complication rates, and a longer recovery period than new minimally invasive procedures. Other clinics use robotics, which require more incisions and more scarring. If your physician recommends these options, consider seeking out a second opinion before agreeing to the surgery.
How does he/she perform fibroid removal?
There are two main surgical treatment options for removing fibroids: a myomectomy, which only removes the fibroids, and a hysterectomy, which removes the uterus and fibroids. The treatment should be selected based on the woman’s individual health concerns and desire to have children in the future. Within those two surgical options, OB-GYNs also perform a wide range of surgical techniques with significantly different incision lengths, recovery times, and risk of complications. For example, unlike standard laparoscopic and robotic techniques, The Center for Innovative GYN Care’s LAAM-BUAO myomectomy procedure has no limitation to the location, size and quantity of fibroids it can safely remove. Other procedures can only remove smaller fibroids and those found in a limited number of locations. Be sure your physician is using the latest advances in minimally invasive GYN surgery, as explained in our myomectomy and hysterectomy pages.
Does he/she recommend an open myomectomy surgery?
Open myomectomies are still the mostly commonly performed surgery to remove fibroids, but the major disadvantage with this type of approach is that it requires a much larger incision than new, minimally invasive techniques, resulting in longer hospital stays, more pain during recovery and longer recovery times – patients often need six to eight weeks to recover. A LAAM procedure, however, can be conducted in an outpatient setting with no hospital stay, and patients generally recover in 10-14 days.
How many times has the physician performed this procedure?
On average, an OB-GYN performs 27 hysterectomies per year, while the average GYN surgeon performs 400 or more hysterectomies. Since a heavy surgical volume is necessary to develop and maintain surgical expertise, be careful to select a surgeon who specializes in performing GYN surgery.
What have other patients experienced after this procedure?
Robotic, open and conventional laparoscopic surgeries can lead to longer recovery times, increased blood loss and larger scars than newer procedures. Make sure your surgeon is trained in the latest minimally invasive techniques, such as The Center for Innovative GYN Care’s DualPortGYN, that prevent injury to the pelvic structures and minimize blood loss – resulting in reduced complication rates and improved recovery times.
Has the physician received fellowship training in minimally invasive GYN surgery?
While most OB-GYNs are highly trusted generalists, they spend most of their time focusing on obstetrics and basic GYN care and therefore, perform hysterectomy and other specialized GYN surgeries rarely. Be sure to choose a surgeon who has received comprehensive training and performs many minimally invasive surgeries each year.
Will the physician use power morcellation to remove tissue during the surgery?
While most OB-GYNs are highly trusted generalists, they spend most of their time focusing on obstetrics and basic GYN care and therefore, perform hysterectomy and other specialized GYN surgeries rarely. Be sure to choose a surgeon who has received comprehensive training and performs many minimally invasive surgeries each year.
Will the physician use robotics to assist with the surgery?
Although the American Medical Association and other leading medical societies have issued statements discouraging robotic techniques due to dramatically higher costs to patients without any medical advantages, robotics continue to be used in hysterectomy and other GYN surgeries. This is because robotic procedures “enable” an OB-GYN not well trained in laparoscopic GYN surgical techniques to complete a hysterectomy through a “minimally invasive” approach. This is why women need to ask if robotics will be used during a GYN surgery and to seek a specially trained surgeon able to perform the latest minimally invasive surgical techniques, such as DualPortGYN and retroperitoneal dissection that do not use robotics.
What is the anticipated recovery time?
New minimally invasive techniques require, on average, only a week to recover. Other procedures such as open abdominal surgery can take up to 8 weeks.
What are my other surgical options?
If your physician recommends an open or robotic procedure, ask why he or she would not recommend a conventional laparoscopic procedure or a newer technique like DualPortGYN or the LAAM-BUAL.
GYN Surgery Glossary of Terms
Adenomyosis
Adenomyosis is a condition that occurs when cells that normally line the inside of the uterus (endometrium) grow into the muscular wall of the uterus (myometrium).
Adenomyosis can result in an enlarged uterus and cause very painful periods and heavy bleeding. It typically affects women in their 40s and 50s. Risk factors include childbearing, previous uterine surgery, short menstrual cycles, and beginning menstruation at an early age. When women are not finished with childbearing, adenomyosis is treated temporarily with medication, hormone suppression and birth control. The only cure for adenomyosis is a hysterectomy.
The bladder is a hollow, muscular structure that collects urine excreted by the kidneys before urine is excreted through the urethra and out of the body.
Bladder
The bladder is a hollow, muscular structure that collects urine excreted by the kidneys before urine is excreted through the urethra and out of the body.
Cervical Dysplasia
Cervical dysplasia is a precancerous condition in which abnormal cell growth occurs on the surface of the cervix, the opening between the uterus and the vagina. It usually occurs with no symptoms. The condition is often discovered through a routine Pap test and is most common in women under age 30, although it can develop at any age. While cervical dysplasia can go away on its own, women who go undiagnosed or do not receive appropriate care are at higher risk of developing cervical cancer. Depending on the form of the dysplasia, treatment may entail cryosurgery to remove highly localized areas of precancerous cells or early stage cervical cancer, loop electro-surgical excision procedure (LEEP) or cold knife conization (CKC).
Cervix
The cervix is the lower, narrow part of the uterus (womb) and forms a canal that opens into the vagina, which leads to the outside of a woman’s body.
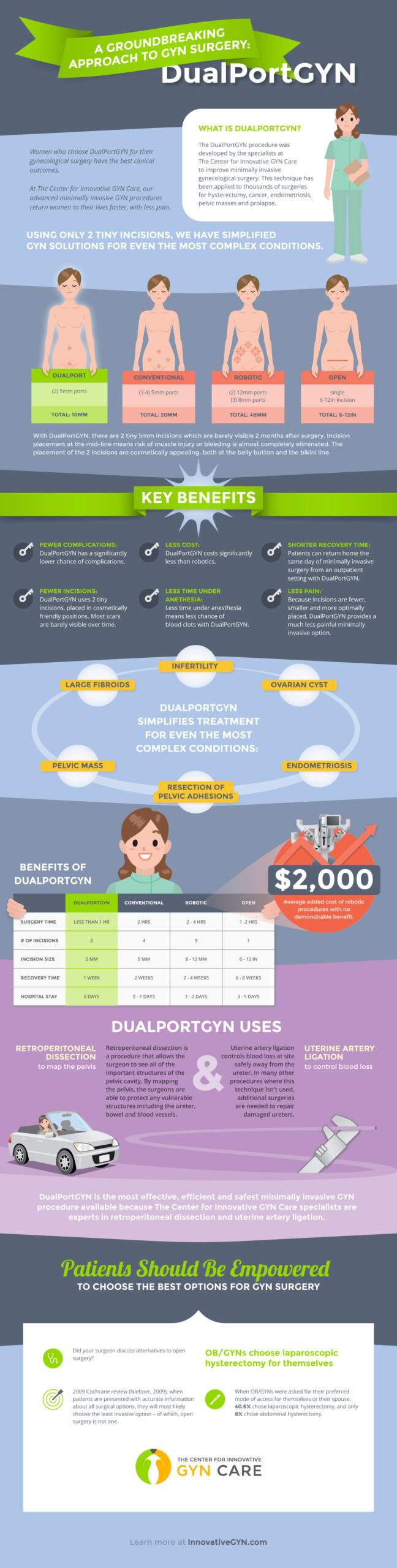
DualPort GYN
Endometriosis
Endometriosis occurs when the endometrial cells (uterine lining cells) exist outside of the uterus. It affects one in ten women worldwide. Endometrial cells can also occur in fallopian tubes or ovaries – and rarely on surrounding organs in the abdomen, such as the intestines, bladder or rectum. Endometrial cells have been detected in all areas of the body. These displaced cells act as though they were part of the uterus, by swelling and thickening, then bleeding with each menstrual cycle. But because the cells have no way to exit the body, they become trapped and the surrounding tissue becomes irritated, leading to adhesions and scar tissue that worsens over time. The result can be pelvic pain, “killer cramps,” long and heavy periods, pain associated with sexual activity and infertility. Currently, the best-known treatment for endometriosis is a procedure called “laparoscopic excision surgery,” in which a trained GYN surgeon removes the endometrial lesions through tiny incisions in the abdomen. Many surgeons believe that endometriosis is cured with a hysterectomy. While that can be a significant improvement to controlling pain, unless all of the endometriosis is removed, it can continue to cause pain.
Fallopian Tube
Fallopian tubes are two, thin muscular channels in the female reproductive system that connect the ovaries to the uterus. They create the path that the eggs use to travel from the ovaries to the uterus.
Fibroids
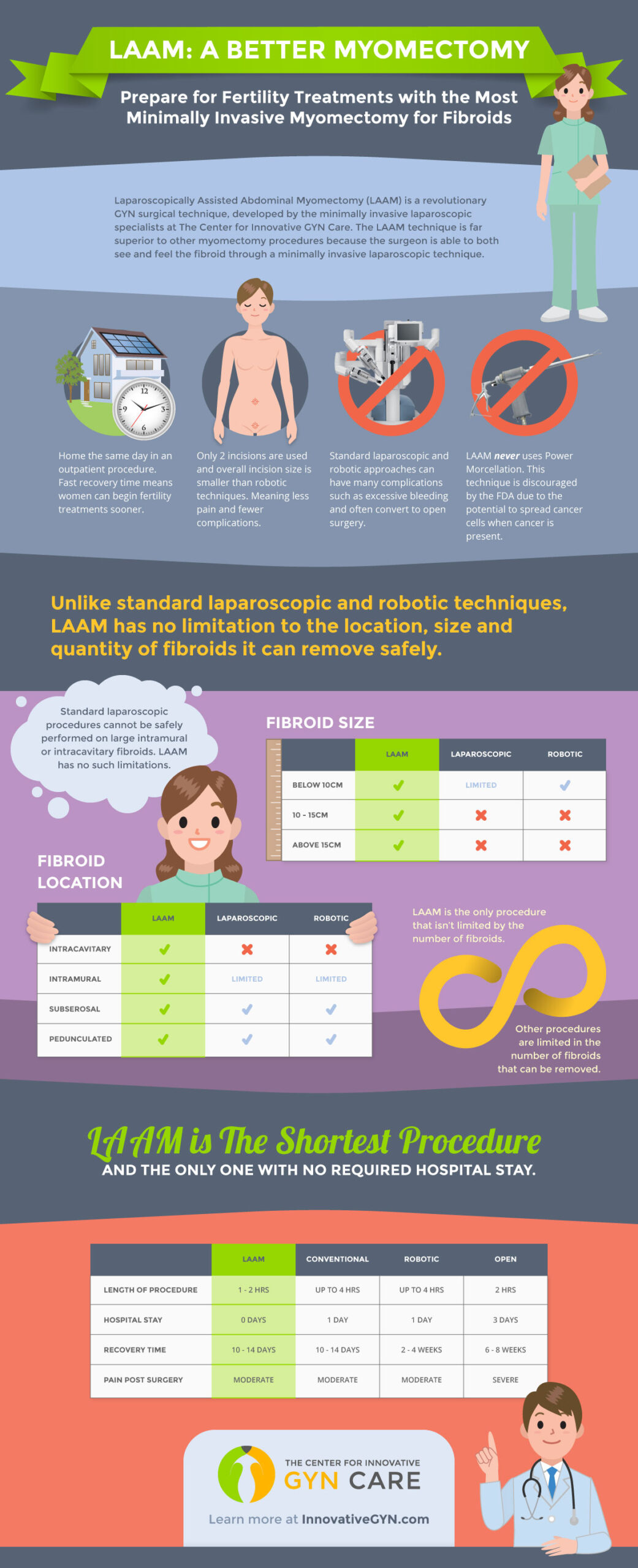
Uterine fibroids (also called myomas or leiomyomas) are noncancerous tumors that originate in the smooth muscle cells inside the wall of the uterus. Incredibly common, about 30% of women will get fibroids by age 35, and about 70-80% will do so by age 50, African American women have fibroids two to three times more often than Caucasian and Hispanic women. Fibroids can grow as either a single tumor or in clusters, both of which can vary in size from as small as an apple seed to a very large growth. As such, they can change the shape or size of the uterus and sometimes the cervix. Fibroids can cause heavy bleeding during a woman’s period that can bring about anemia. It can also cause abdominal pain or pressure, constipation, incontinence, frequent urination, pain during intercourse, and lower back pain. Fibroids can also cause reproductive problems, including infertility and miscarriage. Among the treatment options for uterine fibroids are hormone therapy, radiological treatment and myomectomy, a surgery which is either preformed as open abdominal surgery or through minimally invasive laparoscopic surgery. One of the newest and most successful types of minimally invasive laparoscopic surgery is called LAAM-BUAL, which removes fibroid tissue of any size using a “mini” incision at the bikini line.
GYN Surgical Specialists VS. Generalists
GYN surgical specialists are fellowship trained in minimally invasive laparoscopic techniques. These specialists only focus on GYN surgery, perform a higher volume of cases, more difficult cases, and use techniques and procedures learned in their training to complete surgeries more efficiently with lower complication rates.
Hysterectomy
A hysterectomy removes a woman’s uterus and cervix ONLY, and does not include removal of the ovaries. (The removal of the ovaries and tubes are a procedure separate from hysterectomy called an oopherectomy. See Oopherectomy below.) In all cases, menstruation stops and a woman loses the ability to bear children. Hormone production is sourced at the ovaries, and is not affected by hysterectomy. Menopause or “the change” does not occur after a hysterectomy is performed. This means that menopausal symptoms such as hot flashes, night sweats, mood swings, anxiety, depression, osteoporosis (bone loss), vaginal dryness, and sexual dysfunction will NOT usually occur with hysterectomy. Hysterectomies are mostly performed to remove fibroids, for severe endometriosis and adenomyosis, and for severe bleeding problems. Precancerous and cancerous problems of the cervix and uterus are also treated with hysterectomy. Although many women (45%) still undergo invasive open abdominal hysterectomy in a hospital setting, new forms of laparoscopic hysterectomy are less invasive, leave little visible scarring have a shorter recovery period, and allow the patient to go home the same day. This includes DualPortGYN, a technique that allows a surgical specialist to perform a hysterectomy laparoscopically through two tiny ports – one at the belly button and the other at the bikini line.
Hysteroscopy
Performed in the office or in the operating room, a hysteroscopy is a procedure in which a long thin camera (scope) is inserted into the uterus to evaluate the uterine cavity. For diagnostic purposes, the scope is inserted through the cervical canal into the uterine cavity to detect intrauterine fibroids and adhesions, endometrial polyps and potentially malignant masses. Other types of hysteroscopy are performed under anesthesia in a hospital operating room to remove fibroids, polyps or adhesions. Hysteroscopy is often performed with a D&C;, an abbreviation for Dilation and Curettage, which refers to the dilation of the cervix and scraping (curettage) of the uterine lining to obtain a sample for analysis or to stop bleeding.
LAAM-BUAO
Board certified GYN surgeons at The Center for Innovative GYN Care have developed a pioneering surgical approach called LAAM-BUAO, which takes the best elements of both laparoscopic and open approaches for fibroid removal – myomectomy. LAAM (Laparoscopic Assisted Abdominal Myomectomy) entails two small incisions, one at the belly button and one at the bikini line, and it can be performed on any patient regardless of fibroid size, number, or location. BUAO (Bilateral Uterine Artery Occlusion) is the blockage of the uterine artery during the procedure to control bleeding. Due to the advantage of the surgeon being able to feel all of the fibroids, LAAM is the most thorough minimally invasive technique used for a myomectomy. Most LAAM procedures are done in an outpatient setting, and patients are able to return to their lives sooner than with open procedures.
Interstitial Cystitis
Interstitial cystitis (IC) is also called painful bladder syndrome. IC is a chronic condition involving bladder pressure, bladder pain and spasms, and sometimes severe pelvic pain. Additional symptoms include urinary frequency, urgency, frequent urination at night and painful intercourse. IC affects between 3% and 6% of American women and can be debilitating enough to disrupt home and work life. Treatment options depend on the severity of the symptoms and may include a change in diet, oral medications, nerve stimulation and different types of surgery for people with severe pain or for those whose bladders can only hold a small volume of urine.
Laparoscopy
Laparoscopy is a type of surgery in which the physician operates through a small abdominal incision using a long, thin instrument that contains a tiny video camera (laparoscope). The camera sends images to a monitor screen to help guide the surgeon during the surgery.
Laparoscopic Supracervical Hysterectomy (LSH)
In this surgical procedure, a laparoscope guides the removal of the uterus but leaves the cervix (Supra means above). However, the procedure is normally performed with a power morcellator, a device that contains tiny motorized blades that do much of the cutting involved in many laparoscopic and robotic surgeries. Three to four incisions are used, ranging in size from 5 mm to 10mm, with at least one 12 mm incision for the power morcellator. Recently, the Food and Drug Administration (FDA) issued warnings against the use of laparoscopic power morcellation when women undergo hysterectomies due to the potential of morcellators to scatter undetected uterine cancer cells through the abdomen and pelvis during surgery.
Laparoscopically Assisted Vaginal Hysterectomy (LAVH)
Laparoscopically assisted vaginal hysterectomy (LAVH) is a surgical procedure that uses a laparoscope to guide the removal of the uterus and/or fallopian tubes and ovaries through the vagina. Through this surgical procedure, three to five ports are located in the pelvis, ranging in size from 5 to 10 millimeters. Although the scars, pain and recovery time from LAVH are usually significantly less than an abdominal surgery, LAVH can be a longer operation and more expensive than a vaginal hysterectomy and other minimally invasive laparoscopic surgical options.
Myomectomy
A myomectomy is a surgical procedure to remove uterine fibroids without removing the uterus. Depending on the location of the fibroids, the myomectomy can be done through the pelvic area or through the vagina and cervix. Removing fibroids may enable a woman to get pregnant after the surgery
Oophorectomy
An oophorectomy is the surgical removal of an ovary or both of the ovaries. It is usually performed with the removal of the fallopian tubes in a salpingo-oopherectomy procedure. A bilateral oophorectomy (both ovaries and fallopian tubes) is most often performed to either remove or prevent ovarian cancer. It can also be performed to treat ovarian cysts when the risk of cancer is higher.
Ovarian Cyst
An ovarian cyst is an accumulation of fluid within an ovary that is surrounded by a thin “shell” and can be as small as a pea or become so large that a woman looks pregnant. Occurring most frequently during a woman’s reproductive years, ovarian cysts can cause pain and bleeding and may be an early form of ovarian cancer. In situations where the cyst is large, causes pain or bleeding, or may be cancerous, physicians may recommend surgical removal.
Ovarian Cystectomy
Ovarian cystectomy is a minimally invasive surgical procedure that uses laparoscopy to remove an ovarian cyst while still preserving the ovary so women can remain fertile. However, not all women are candidates for ovarian cystectomy, especially if the cyst is very large, the ovary is twisted due to the cyst or malignancy is suspected. In post-menopausal women, removal of the ovary (oophorectomy) is preferred as the risk of malignancy is greater.
Ovary
The ovary is one of a pair of female reproductive glands located in the pelvis, one on each side of the uterus. Ovaries produce eggs and female hormones.
Pelvic Organ Prolapse
Pelvic organ prolapse, is a type of pelvic floor disorder. This occurs when pelvic organs (bladder, rectum or uterus) descend into or outside the vaginal canal or anus. Symptoms can include pelvic pressure, pulling or stretching in the groin area, a low backache, painful intercourse, spotting or bleeding, urinary problems, difficulty with bowel movements, and the feeling that something is falling out of the vagina. In most cases, the cause is pregnancy and childbirth but the disorder can also result from obesity, respiratory conditions with a chronic, long-term cough, constipation and pelvic organ cancers. Depending on the severity of the condition, there are a number of treatment options, including surgery either to repair the affected tissue or remove the organ, which can include hysterectomy. For bladder and rectal prolapse, surgical repairs are performed through a vaginal approach.
Resection of Endometriosis
Resection of endometriosis refers to the removal (excision) of endometriotic implants. This is a type of conservative management of endometriosis. The goal of conservative surgery is to improve symptoms while preserving the uterus, tubes and ovaries as much as possible. This is usually done for women who are not yet finished with childbearing or who have milder disease. Conservative surgery improves pain (80 percent of women reported improvement in their symptoms six months after surgery), but it does not cure endometriosis. Forty to 80 percent of women will have a recurrence of pain within two years of surgery. Following conservative surgery with medical management can help to limit the recurrence of endometriosis and extend the length of pain control.
Retroperitoneal Dissection (RPD)
Retroperitoneal dissection, or RPD for short, is an important technique in surgery. By going beneath the peritoneum (membrane) that surrounds the pelvic organs, RPD gives the surgeon a clear view of the pelvic cavity to “map” the entire area. The surgeon is able to see all of the critical anatomy that surrounds the pelvic organs and can avoid potential injury to nearby structures, such as the ureter, bladder, and large blood vessels during GYN surgery. This makes it possible to perform minimally invasive laparoscopic surgeries more quickly and with less blood loss, smaller incisions, and faster recovery than standard laparoscopic, robotic, or open surgical procedures for fibroids, endometriosis, pelvic masses, prolapse, and cancer. However, to perform RPD, surgeons require special training. Currently, DualPortGYN is the only laparoscopic procedure that routinely uses retroperitoneal dissection in GYN surgery.
Robotically Assisted Laparoscopic Hysterectomy (Robotics or RALH)
In a robotically assisted laparoscopic hysterectomy, the surgeon uses a robot to assist in the removal of the uterus and cervix through five laparoscopic ports in the abdomen. The robot’s movements are controlled from a computer station in the operating room, providing the surgeon with a 3D vision system, but without the tactile feel associated with other laparoscopic surgical methods. RALH has been widely promoted as enabling surgeons to get into tiny spaces more easily and have a better view of the operation than with conventional laparoscopic surgery. However, numerous scientific papers find that robotic hysterectomy has no advantage over laparoscopic hysterectomy and is significantly more expensive. Based on these conclusions, the American College of Obstetricians and Gynecologists declared that robotic surgery “is not the only or the best minimally invasive approach for hysterectomy,” nor is it “the most cost-efficient.”
Total Laparoscopic Hysterectomy (TLH)
A total laparoscopic hysterectomy is a procedure whereby the uterus and cervix are removed through laparoscopic ports in the abdomen. Compared to the traditional abdominal hysterectomy, TLH reduces blood loss and postoperative pain and shortens the hospital stay. However, TLH often entails the use of a power morcellator, a device that contains tiny motorized blades that do much of the cutting involved in many laparoscopic and robotic surgeries. Recently, the Food and Drug Administration (FDA) issued warnings against the use of laparoscopic power morcellation when women undergo hysterectomies due to the potential of morcellators to scatter undetected uterine cancer cells through the abdomen and pelvis during surgery.
Total Vaginal Hysterectomy (TVH)
A total vaginal hysterectomy is a procedure by which the uterus and cervix are surgically removed through an incision deep within the vagina. As a minimally invasive form of hysterectomy, TVH typically has the fastest recovery, lowest cost, and comparable if not fewer complications than robotic or standard laparoscopic hysterectomy. However, to perform TVH, surgeons must perform blind as no laparoscopic tools are used to see the uterus. Moreover, the method has limited use as TVH cannot be performed if the uterus is enlarged. Studies comparing TVH to the DualPortGYN procedure have shown clearly that the DualPortGYN approach provides a faster recovery, less blood loss and complications, at a lower cost than the vaginal approach.
Ureter
A part of the urinary tract, the ureter is a muscular duct or tube that carries urine from the kidney into the bladder. Injuring the ureter is one of the most serious complications of GYN surgery.
Uterine Artery Ligation or Occlusion
Uterine artery ligation or occlusion controls blood loss safely away from the ureter, which can often be damaged in laparoscopic surgery, including robotic surgery. In procedures where this technique isn’t used, it is often necessary to have additional surgery to repair damaged ureters. Ligation is used for hysterectomy, and for myomectomy for women who wish to retain their uterus, but no longer wish to have children. Occlusion is used for myomectomy for women who still wish to be able to conceive a child.
Uterus
Often called the womb, the uterus is a hollow, muscular organ in the lower part of a woman’s body in which a fertilized egg implants and develops into a fetus.
Vagina
The vagina is a muscular passage that connects the cervix with the outside of the body.